






![]()

Renal colic
17.12.2023Inflammation of the bladder
18.12.2023BLOG OF DOCTOR SERGII LYULKO
All about cystitis.
How to treat and how not to treat cystitis!
Cystitis is not scary when you don’t have it!


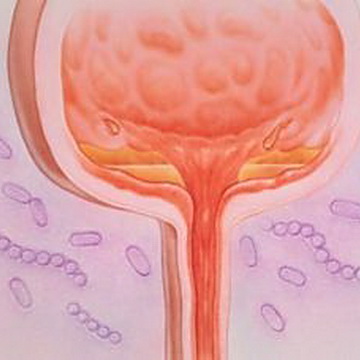

Cystitis — inflammation of the mucous membrane of the bladder, which is accompanied by dysfunction of the bladder and changes in urine sediment.
Despite the fact that cystitis affects women, men and children, urologists often say Cystitis is considered a “women’s disease,” and here’s why:
- Every third woman under 24 years of age suffers acute cystitis at least once;
- 40% of cases of acute cystitis are accompanied by the presence of blood in the urine;
- Every second woman suffers from acute cystitis throughout her life;
- Acute cystitis is accompanied by symptoms for 6 days, limits activity for 2.5 days and limits ability to work for 10 hours;
- On average, the symptoms of cystitis disappear in 2-3 days;
- The most common consequence of cystitis in women is ascending pyelonephritis (inflammation of the kidneys);
- In the period from 20 to 50 years, women suffer from acute cystitis 50 times more often than men;
- The prevalence of acute and chronic cystitis in Ukraine is 314 and 135 patients per 100,000 population, respectively.
Pathogenesis of cystitis
Impaired urination rhythm can affect the development of cystitis in women. This is often associated with the bad habit of not emptying the bladder on time for various reasons.
Cystitis can be the first manifestation of pyelonephritis, urolithiasis, developmental anomalies or oncological processes.
The infectious agent of most cystitis is Escherichia coli (E. coli) in 80%, saprophytic staphylococcus (St. Saprophiticus) in 11%, as well as Klebsiella, enterococci, Proteus, mycoplasma and viruses .
Fixation of the pathogen to the mucous membrane of the bladder occurs with increased pressure in the bladder and disturbances in the urodynamics of the lower urinary tract, which in turn causes venous stagnation, ischemia - circulatory disorders, damage to the walls of the bladder and their degenerative changes.
Hypothermia can also cause ischemia of the bladder mucosa.
Conditions for the occurrence of cystitis:
- Difficulty urinating;
- Pathogenic microorganisms;
- Irregular urination rhythm in women;
- Disturbance of local blood circulation in the wall of the bladder (for example, during hypothermia).
Infection enters the bladder in the following ways:
The Ascending Path – through the urethra the infection rises up into the bladder. This route is dominant in women due to the wider and shorter urethra.
Downward path – the infection “goes down” from the kidneys, i.e. from top to bottom (for example, with pyelonephritis);
Contact path – in direct contact of the bladder with the source of inflammation (for example, with appendicitis, parametritis, prostate abscess).
Lymphogenic pathway – the infectious agent is transferred from neighboring pelvic organs with lymph (in inflammatory diseases of the female genital organs, rectum, prostate);
Hematogenous route – the pathogen enters the bladder from distant lesions with blood (tonsillitis, cholecystitis, caries, etc.)
Clinical classification cystitis:
1. During the course of the disease :
Acute cystitis - a sudden onset (within a few hours), occurs with pronounced characteristic symptoms and, with timely treatment, ends in recovery.
Postcoital cystitis – cystitis, which develops within 24 hours after sexual intercourse.
Chronic cystitis - recurrent cystitis with a frequency of at least three episodes of exacerbation per year or two episodes during the last 6 months, however, the symptoms may not be as severe as with acute cystitis.
2. According to the pathogenetic principle , primary and secondary cystitis are distinguished, which occurs against the background of various diseases and anomalies of the bladder or genital organs (for example, sclerosis of the bladder neck, urinary stones bladder, prostate hyperplasia, urethral stricture, etc.)
In men, cystitis is always secondary and is often part of the symptom complex of acute prostatitis.
3. According to etiology and pathogenesis:
A) Infectious cystitis:
Specific cystitis - for example, tuberculosis;
Nonspecific cystitis – bacterial, viral;
Parasitic cystitis - with schistosomiasis;
B) Non-infectious cystitis:
Chemical cystitis develops when a chemically aggressive liquid is introduced into the bladder, which often leads to the development of one of the most severe forms of cystitis - necrotic;
Radiation cystitis occurs when the bladder is exposed to radiation therapy for oncological processes in the pelvic organs (cancer prostate, cervical cancer);
Drug-induced cystitis is caused by taking cyclophosphamide and certain chemotherapy drugs that irritate the bladder mucosa;
Allergic cystitis – inflammation that is associated with an allergic reaction to substances excreted in the urine. Typically, such patients have a history of allergic reactions.
4. By localization and extent of the inflammatory process:
Diffuse – the entire mucous membrane of the bladder is inflamed;
Focal – inflammation of mucous membranes;
Trigonite – inflammation of the bladder neck (Lieto's triangle).
5. According to the depth and nature of pathomorphological changes, the following are distinguished:
Acute cystitis - catarrhal, follicular, hemorrhagic, ulcerative and necrotic;
Chronic cystitis - encrusting, polypous, cystic, ulcerative and interstitial - which is based on a deeper (interstitial) inflammation of the bladder tissue.
According to the European and American classifications, cystitis is not distinguished separately, but speaks of uncomplicated and complicated infections of the lower urinary tract, which includes the urethra.
Acute uncomplicated cystitis - acute, single, or recurrent cystitis in non-pregnant women before menopause, in who do not have anatomical or functional disorders of the urinary tract, without concomitant diseases.
Corresponds to the classification - primary acute infectious nonspecific (bacterial) cystitis - can only occur in women.
Complicated lower urinary tract infections - develop in patients who have common risk factors (eg, diabetes mellitus or immunosuppression) or specific anatomical or functional disorders of the urinary tract (obstruction, incomplete urination) make eradication of infection more difficult than uncomplicated urinary tract infections.
Corresponds to the classification of secondary acute infectious nonspecific (bacterial) cystitis.
Factors contributing to the development of acute cystitis:
- Chronic emotional stress;
- Insufficient fluid intake;
- Use of spermicides;
- Sexual intercourse with a new sexual partner;
- Frequent change of sexual partners;
- Sexually transmitted infections;
- History of maternal urinary tract infections;
- An episode of urinary tract infections in childhood;
- Decreased lubrication during sexual intercourse.
Factors contributing to the development of chronic
cystitis:
- Urinary incontinence;
- Atrophic vaginitis due to estrogen deficiency;
- Cystocele;
- Increase in residual urine volume;
- Bladder catheterization;
- Impaired functional state of the urinary tract;
- Concomitant diseases of the genitourinary system;
- Obstruction at any level of the urinary tract;
- Urinary tract infections in men;
- Foreign bodies (eg bladder stone);
- Pregnancy;
- Incomplete emptying of the bladder;
- Diabetes mellitus;
- vesicoureteral reflux;
- Immunosuppression;
- Recent instrumental interventions;
- Nosocomial infections.
Lifestyle that can influence the development of cystitis:
Sedentary lifestyle Sedentary work for 8-10 hours a day is now common. As a result, venous blood stagnates in the pelvis, which contributes to the development of infection.
Irrhythmia of urination in women. Scientists have proven the connection between this fact and cystitis. Even slight containment increases the chance of infection of the blister.
Wearing tight underwear and tight clothing that tightly fits the female form is an indirect culprit of cystitis. The result is stagnation of blood in the pelvis.
Hypothermia. The cause of summer hypothermia is air conditioning or work in freezing shops, and winter - out-of-season clothing or cold seats.


Diagnostics of cystitis
The urologist collects complaints, medical history, performs a general examination and prescribes additional examinations.
Symptoms of cystitis:
- pain above the pubis;
- painful urination;
- frequent urge to urinate with small portions of urine;
- cutting and burning when urinating;
- sharp urge to urinate;
- cloudy urine and sometimes mixed with blood;
- no vaginal discharge or other symptoms of vaginitis.
General urine analysis – mandatory analysis - the urine is cloudy, with flakes and an unpleasant odor, an increased number of leukocytes, bacteria, and red blood cells. If the urine test is normal, then the diagnosis of cystitis is practically excluded.
Complete blood test – in the presence of uncomplicated cystitis remains normal, but with the addition of pyelonephritis, the total number of leukocytes increases and the percentage of band leukocytes increases.
Urine culture with determination of sensitivity to antibiotics in acute primary cystitis is not performed , but for chronic cystitis and cystitis in pregnant women – Necessarily! It is based on the results of the antibiogram that the antibiotic is selected.
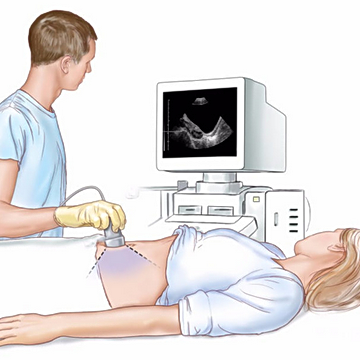
Ultrasound to assess the condition of the kidneys, bladder, and pelvic organs. Usually, with cystitis, ultrasound shows a thickening of the bladder wall and sometimes a suspension in the bladder cavity.
Cystoscopy – This is an examination of the bladder cavity using a special instrument – a cystoscope, which is inserted into the bladder through the urethra (urethra).
The cystoscope has a camera through which the image is displayed on a screen. The urologist assesses the condition and changes in the bladder mucosa, bladder capacity, how the orifices of the ureters are located, whether there are any additional formations, leukoplakia of the bladder or stones.
Cystoscopy is performed only for chronic cystitis, for cystitis that lasts more than 2-3 weeks , and after hemorrhagic cystitis.
For women with chronic and acute cystitis, which is accompanied by vaginal discharge, a mandatory examination by a gynecologist and examination for sexually transmitted infections are necessary.
Differential diagnosis of cystitis is carried out with:
- Stone of the intramural ureter;
- Bladder cancer;
- Urethritis ;
- Diverticulum of the bladder;
- Diseases of the pelvic organs;
- Hyperplasia and prostate cancer;
- Appendicitis.
A competent diagnosis can only be made by a doctor -urologist.


Treatment of acute and chronic cystitis
Treatment of cystitis is mainly carried out on an outpatient basis, but in severe cases, inpatient treatment may be required.
We will discuss below the treatment of acute and chronic infectious (bacterial) cystitis - which is the most common form of cystitis in urological practice.
IMPORTANT TO KNOW!!!
MAIN Treatment of infectious cystitis - Antibacterial, that is, you need to take antibiotics!!!
For chronic cystitis and cystitis in pregnant women– The antibiotic is selected based on the results of urine culture and determination of the sensitivity of bacteria to antibiotics, which is mandatory.
Antibiotics for uncomplicated cystitis are prescribed for up to 5 days, and for complicated cystitis, sometimes from 7 to 14 days.
BUT OFTEN WOMEN DO SELF-MEDICATION!
"I asked a friend, they advised me at the pharmacy…."
Before seeing a urologist, many women have been taking herbal medicines and dietary supplements for several days and sometimes weeks.
The problem is that herbal preparations only reduce symptoms and do not affect the severity of inflammation in the bladder!
It’s like taking a painkiller for a headache caused by high blood pressure, and not drugs to lower blood pressure - and as a result, a stroke or heart attack!!!
With cystitis, the situation is similar - women who take only herbal medicines come with pyelonephritis - inflammation of the kidneys, which requires longer treatment and often in a urological hospital.
If a woman experiences weakness, symptoms of intoxication, and an increase in body temperature due to cystitis, then most likely kidney inflammation has occurred.
In addition to antibacterial therapy for cystitis, it is recommended:
Peace ;
Vegetable and dairy nutrition and exclude from the diet - hot seasonings, spices, canned food, meat broths;
Taking enough fluid – diuretic herbs, teas, jelly, cranberry juice, mineral waters;
Thermal procedures (contraindicated for hemorrhagic cystitis): sitz baths 38-40 C every day for 5-9 days; dry heat (heating pad) on the bladder area;
Physiotherapeutic procedures – UHF, UV, laser therapy – on the bladder area;
Anspasmolytic and painkillers : no-spa, spasmalgon, suppositories with belladonna extract, ketanov, diclofenac, etc.;
Hemostatics (hemostatic agents) - for severe hemorrhagic cystitis. Well known to women – sodium ethamsylate, Dicinone, nettle decoctions, nettle extract suppositories and others;
Instillation into the bladder of substances that help restore the bladder mucosa - in case of chemical, radiation and chronic cystitis;
Prophylaxis with immunoactive drugs , for example, Uro-Vax, has shown high clinical effectiveness and is recommended for women with acute and chronic recurrent cystitis;
Phytopreparations (cranberry, D-manose, bearberry, etc.) – taken only while taking antibiotics to reduce the severity of symptoms– for example, SolUroDuo, Canephron, Krenfors, Cystinol Acute and others.
IMPORTANT!!!
PHYTOMEDICATIONS DO NOT TREAT CYSTITIS , AND REDUCE THE SYMPTOMS OF CYSTITIS!!!
DO NOT SELF-medicate !
For radiation cystitis hormonal, desensitizing drugs and drugs that increase reactivity are prescribed to reduce the inflammatory process;
Interstitial cystitis requires specific treatment, which I will talk about in the following articles.
Cystitis in pregnant women – one of the most common pathologies.
Often it is completely asymptomatic, but it significantly increases the risk of premature birth and fetal development retardation.
Cystitis in pregnant women is treated with antibiotics, which are as safe as possible for the fetus.
Antibiotic - selected based on the result of urine culture with antibiogram.
Important!!!
Pregnant women for the prevention and treatment of cystitis most herbal remedies cannot be used!!!
Every pregnant woman should be under the supervision of an obstetrician-gynecologist and undergo timely screening, including a urine test.
If cystitis develops, the urologist prescribes treatment in a timely manner.
Cystitis in women who are breastfeeding.
If cystitis occurs in women who are breastfeeding, then during the period of antibiotic treatment the child must be switched to formula feeding.
This must be done because that the antibiotic will get into the baby's milk and may cause intestinal problems or allergies.
Prevention of cystitis:
- Effective treatment of acute cystitis under the supervision of a urologist;
- Timely treatment of inflammatory diseases of the genital organs and sexually transmitted infections;
- Rehabilitation of inflammatory processes in the kidneys and timely treatment of urination disorders;
- Do not use scented soaps, gels or bubble baths for external genital hygiene;
- If you have a sedentary job, then get up, walk, and squat at least every hour and a half. This will help you prevent cystitis and improve the health of the lumbar spine;
- If you want to urinate, go to the toilet;
- Take a shower rather than a bath;
- Wear looser clothing;
- Follow the rules of personal hygiene;
- If you have insufficient lubrication, use water-based lubricants;
- Keep your feet warm and, most importantly, do not sit on the cold;
- Drink enough table water;
- Do not apply deodorants to the external genitalia, even those intended for private parts, powder, etc.
Despite all the apparent “safety” at first glance, cystitis can lead to serious complications.
If you want to undergo a full examination and receive professional urological help for cystitis and other urological diseases, sign up for a consultation with me in a way convenient for you.
This article is purely popular science!
The described treatment options are prescribed only by a urologist.
Many drugs have contraindications!
Self-medication is dangerous for your health!


